What exactly is cholesterol?
Cholesterol is often portrayed as the "number one enemy" of heart health. However, science tells us that this molecule is, first and foremost, an essential element for our life. Without cholesterol, our body simply could not function.
Cholesterol is a sterol, a fatty substance (lipid) that performs vital functions:
- Cell structure: Acts as "cement" for our cell membranes, making them stable yet flexible.
- Nervous system: A fundamental component of myelin, the sheath that covers and insulates our nerves, allowing electrical signals to travel correctly.
- Hormone factory: The raw material from which the body produces essential hormones such as vitamin D, cortisol, testosterone, progesterone, and estrogen.
- Digestion: Without cholesterol, we couldn't produce bile salts, necessary for digesting and absorbing the fats we eat.
Where does it come from? (The diet myth)
Many people think cholesterol depends only on what we eat. In reality:
- 80-90% of cholesterol is produced by the body itself, mainly in the liver and intestine. The brain even produces all the cholesterol it needs on its own.
- Only 10-20% comes from food (eggs, butter, meat, fish).
Our body has a very sophisticated control system: if we eat more cholesterol, the liver produces less; if we eat little, the liver increases production to ensure it never runs out.
Transport in the blood
Being a fat, cholesterol cannot dissolve in blood (which is water-based). To travel, it must be "packaged" in special spheres called Lipoproteins.
- Lipoprotein (a): Lp(a) is associated with increased lifetime cardiovascular risk. The relative risk is multiplicative with other risk factors. Lifestyle modifications have minimal impact on Lp(a) as it is predominantly genetically determined. Specific therapies (e.g., mRNA therapies or small molecule oral inhibitors) are currently being tested in trials.
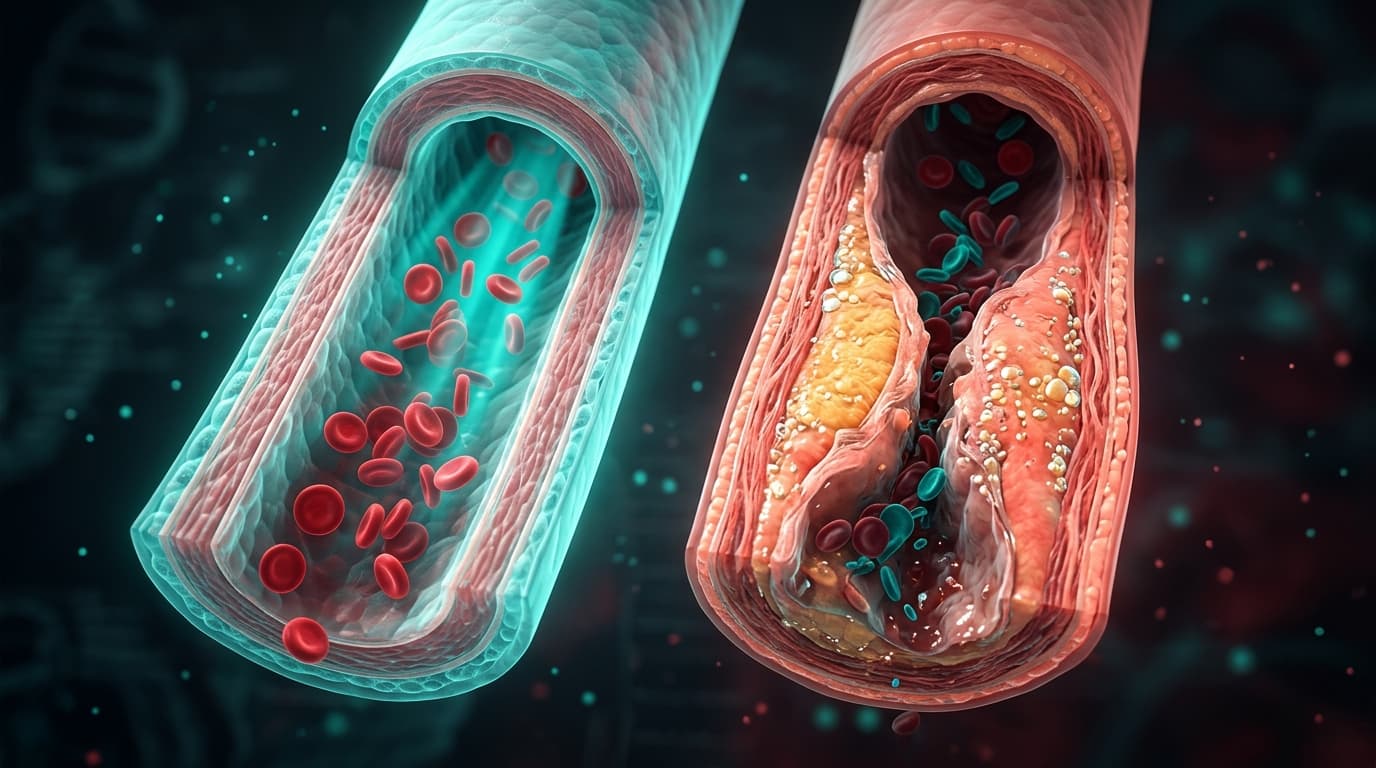
- Low-density lipoprotein (LDL): These particles deliver cholesterol to cells that need it. However, if they are too numerous or too small and dense (small dense LDL - Pattern B), they can be captured by immune cells (macrophages) in blood vessel walls, contributing to plaque formation (arteriosclerosis).
- Very Low-Density Lipoproteins (VLDL): Triglyceride-rich lipoproteins representing about half the myocardial infarction risk associated with apoB-containing lipoproteins. Their atherogenic mechanisms include arterial wall penetration, release of toxic free fatty acids, foam cell formation, and higher cholesterol content per particle.
- Small dense LDL (sdLDL) and oxidized LDL (oxLDL): Modified and highly atherogenic forms of LDL cholesterol, mainly responsible for plaque formation in arteries. sdLDL are particularly predictive of myocardial infarction and peripheral arterial disease.
- Apolipoprotein B: ApoB directly measures the number of atherogenic particles (LDL, VLDL, Lp(a)), providing a more accurate assessment of atherogenic burden than LDL-C. ApoB is standardized and unaffected by fasting status.
- High-density lipoprotein (HDL): Acts as a "scavenger." Collects excess cholesterol from tissues and returns it to the liver to be disposed of through bile.

The bile cycle: natural elimination
The body eliminates excess cholesterol by converting it into bile acids. These are released into the intestine to aid digestion. About 90% of these bile salts are reabsorbed and reused (enterohepatic circulation), while the rest is expelled with feces. This represents the main way to eliminate excess cholesterol from the system.
When should we worry? What affects cholesterol levels?
The medical term for high cholesterol is Hypercholesterolemia. Hypercholesterolemia is a multifactorial condition. Blood fat levels are the result of a complex balance between genetics, daily habits, and even our psychological response to events.
1. Diet: Fats and Carbohydrates Under the Lens
- Saturated Fats: The effect on cardiovascular risk is complex. Studies indicate that the LDL increase is significant mainly when polyunsaturated fat intake is deficient. LDL-C reduction induced by saturated fat restriction mainly affects large LDL particles (less atherogenic), while small dense LDL particles (more atherogenic) are not reduced in most individuals.

- Trans Fats: Much more dangerous, found in margarines and industrial products like chips and biscuits. Their effects include: increased total cholesterol and LDL-C, decreased HDL-C (a unique effect compared to saturated fats).

- The Role of Eggs: Although rich in cholesterol, eggs affect blood levels less than previously thought. A 2020 meta-analysis of over 1.7 million participants showed that moderate egg consumption (up to 1 egg per day) is not associated with overall cardiovascular risk. The quality of eggs is decisive: choose eggs whose first number printed on the shell is 0 (organic farming).
- Sugars and refined carbohydrates: An excessively sugar-rich diet with refined carbohydrates can alter the lipid profile. Excess carbohydrates increase triglyceride synthesis in the liver and promote the shift from LDL "Pattern A" (large, less dangerous particles) to "Pattern B" (small, dense, highly atherogenic particles).

2. Internal medical causes
The American College of Cardiology/American Heart Association and the European Society of Cardiology recommend excluding secondary causes of hypercholesterolemia before diagnosing a primary or genetic dyslipidemia.
Causes of hypercholesterolemia may include:
- Physiological: Menopausal transition, pregnancy (especially third trimester)
- Metabolic factors: Hypothyroidism, obstructive liver disease, chronic kidney disease, nephrotic syndrome, diabetes and insulin-resistant states, uncontrolled hyperglycemia, Cushing's syndrome, anorexia nervosa, obesity
- Medications: High-dose thiazide diuretics, beta-blockers, glucocorticoids, anabolic steroids, estrogens, androgens, atypical antipsychotics, cyclosporine, and others
3. Stress
Psychological stress is a recognized contributing factor that can worsen an already altered lipid profile, reduce the effectiveness of lifestyle interventions, and contribute to residual cardiovascular risk.
Chronic stress seems to influence cardiovascular risk primarily through acceleration of the atherosclerotic process, leading to increased LDL and decreased HDL. The pathophysiological mechanism is secondary to hypercortisolism that generates altered hepatic metabolism.
Acute stress can trigger thrombotic, arrhythmic, or mechanical events in subjects with underlying atherosclerosis, secondary to catecholaminergic peaks with subsequent lipid mobilization.
4. Daily lifestyle
- Physical Activity: Intense exercise significantly increases HDL levels (protective cholesterol). Even a simple consistent walk shows benefits, while sedentary behavior is closely correlated with low HDL levels and obesity.
- Smoking: Smoking is a direct enemy of arteries. It reduces HDL and can increase total cholesterol by up to 17% and LDL by 35%. Smokers have a drastically higher cardiovascular risk.
Guyton and Hall, Textbook of Medical Physiology: Descrizione della sintesi del colesterolo e della sua funzione nelle membrane e nelle guaine mieliniche.
Berg, J.M., et al., Biochemistry: Il ruolo del colesterolo come precursore della Vitamina D e degli ormoni steroidei.
Hofmann, A.F., The enterohepatic circulation of bile acids in health and disease.
Dietschy, J.M., & Turley, S.D., The role of cholesterol in the brain and the mechanism of HMG-CoA reductase feedback.
USDA FoodData Central / Souci-Fachmann-Kraut: Dati sulla concentrazione di colesterolo negli alimenti (Uova, Burro, Carne).
Lewis, G.F., & Rader, D.J., New insights into the regulation of HDL metabolism and reverse cholesterol transport.
Krauss, R.M., Lipoprotein subfractions and cardiovascular disease risk (Differenza tra Pattern A e Pattern B delle LDL).
Austin, M.A., et al., Low-density lipoprotein subclass patterns and risk of myocardial infarction.
Tall, A.R., Cholesterol ester transfer protein and HDL metabolism.
Chiang, J.Y., Bile acid metabolism and signaling in liver disease and metabolic homeostasis.