1. Why has CCTA revolutionized diagnostic cardiology?
Until a few years ago, the only way to study the coronary arteries was through invasive coronary angiography (via catheterization). Angiography, however, only displays the "lumen"—the internal space where blood flows.
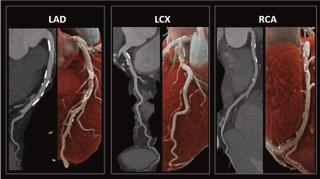
Coronary Computed Tomography Angiography (CCTA) completely changes this perspective: it functions like a three-dimensional radar capable of analyzing vascular wall thickness. This allows for the identification of early atherosclerotic lesions long before they progress to obstruct blood flow.
- The Power of "No": CCTA boasts a Negative Predictive Value (NPV) close to 99%. This means that if the test is negative, the exclusion of coronary artery disease is mathematically definitive and absolute.
- Seeing the Plaque Saves Lives: Long-term data from the landmark SCOT-Heart Trial confirm that CCTA drastically reduces non-fatal myocardial infarction.
🩺 Cardio Insight (For Physicians): The pivotal finding of the SCOT-Heart Trial demonstrates that the reduction in 10-year events is not driven by an increase in preventive revascularizations (stents or bypass grafts), as these rates remained comparable to standard care. The true game-changer is the optimization of medical therapy: directly visualizing plaque—even if non-obstructive—promotes significantly higher adherence to targeted preventive therapy (statines and aspirin), fundamentally altering the natural history of the disease. Clinical efficacy therefore resides in the image itself, combined with its capacity to guide personalized prevention.
2. The ideal patient: when the scan is appropriate (and when it is not)
The flip side of the coin lies in the risk of overdiagnosis and the critical importance of rigorous patient selection.
- Ideal Target: Patients with a low-to-intermediate pre-test probability.
- Technical Limitations: Advanced age, severe obesity, and arrhythmias compromise diagnostic image quality.
Pre-test probability helps clinicians select appropriate candidates for this exam. This probability must be determined by a physician based on symptom type—specifically the characteristics of chest pain—as well as classic cardiovascular risk factors such as smoking, dyslipidemia, arterial hypertension, diabetes, and a positive family history.
CCTA is appropriate only when the pre-test probability is low to intermediate. Conversely, for patients with a very low pre-test probability, additional testing can be safely bypassed, while those with a high pre-test probability should instead be referred for functional testing or directly for invasive coronary angiography. Targeted patient selection is essential to avoid unnecessary invasive procedures.
Technical limitations of the exam
Certain clinical scenarios degrade image quality, rendering the exam non-conclusive:
- Advanced Age: Less indicated in men over 70 and women over 75. Aging increases massive calcifications, which generate beam hardening artifacts that can "blind" the software.
- Cardiac Arrhythmias: Atrial fibrillation or frequent premature ventricular/atrial contractions (PVCs/PACs) create motion artifacts that blur the images.
- Renal Impairment: A reduced glomerular filtration rate (eGFR < 30 mL/min) contraindicates the exam due to the necessity of administering iodinated contrast media.
- Severe Obesity: Excess adipose tissue attenuates the X-ray beam, thereby reducing the image's signal-to-noise ratio.
3. What happens during the exam: preparation and execution
The entire procedure takes approximately 30 minutes and requires strict medical supervision. It is structured into precise steps:
- Preparation
- A peripheral intravenous line is established, and electrodes are applied for continuous ECG monitoring.
- Slowing the Heart Rate: To achieve crystal-clear images, the heart must beat slowly. If the baseline heart rate is above 65 bpm, the patient is administered a beta-blocker prior to entering the scanner.
- Dilating the Arteries: Immediately before the scan, sublingual nitrate spray is administered to maximize coronary artery dilation and optimize luminal visualization.
- Execution
- Acquisition of native (non-contrast) images.
- Injection of intravenous contrast media (calibrated to body weight) followed by the acquisition of the angiographic images.

4. Calcium Score: "The true age of your arteries"
The initial phase of the scan (without contrast) allows for the calculation of the Calcium Score, a numerical value that quantifies arterial calcification. Processed by the software into percentiles, it defines the patient’s true biological coronary age.
The second phase of the scan (with contrast) visualizes the coronaries, analyzing the presence and specific characteristics of atherosclerotic plaques centimeter by centimeter.

Generally, CCTA delineates three clear diagnostic scenarios:
- Calcium Score = 0: Indicates the absence of calcified plaque and is associated with an extraordinarily low rate of cardiac events for many years. In the absence of other clinical indicators, a score of zero may allow patients to avoid or defer statin therapy.
- Non-Obstructive Coronary Artery Disease (Stenosis < 50%): The Calcium Score is > 0 and/or plaques are present that narrow the vessel without blocking blood flow. This scenario dictates aggressive preventive management (lifestyle modifications and targeted pharmacotherapy).
- Obstructive Coronary Artery Disease (Stenosis > 50%): The presence of significant plaques that require further functional evaluation or invasive assessment.
⚠️ Beware of High-Risk Plaques: CCTA does not merely count calcium; it identifies high-risk (vulnerable) plaques. These plaques are characterized by a large, inflamed lipid core (rich in macrophages), thin fibrous caps, or spotty focal calcifications. Identifying and thoroughly describing these features is critical, as they signal the need to heavily intensify the management of cardiovascular risk factors.

5. It is not (yet) a screening tool
The growing inclination to use Coronary CT as a routine check-up must be carefully weighed against non-negligible radiation exposure, potential side effects related to contrast media, and the discovery of incidentalomas (incidental findings). These unexpected findings can trigger an unnecessary cascade of follow-up tests, biopsies, and patient anxiety.
At the same time, Coronary CT stands as an incredibly powerful tool within Precision Medicine. It is not a generic screening to be done "just to be safe." However, when prescribed to the correctly selected patient, it allows clinicians to rewrite the biological destiny of their arteries—preventing a cardiovascular event long before it can manifest.
Newby DE, et al. (SCOT-HEART Investigators). Ten-year outcomes of coronary CT angiography-guided management of patients with stable chest pain. The Lancet, 2024/2025
Magalhães TA. Coronary CT Angiography in 2025: Long-Term Evidence, Artificial Intelligence, and the Photon-Counting Era. ABC Imagem Cardiovasc, 2025
Rajani R, et al. Photon-counting detector CT: the next frontier in cardiovascular imaging. European Heart Journal, 2025
AHA/ACC Guidelines 2025. Guideline for the Management of Patients With Acute and Chronic Coronary Syndromes. Journal of the American College of Cardiology, 2025.
European Society of Cardiology (ESC) Guidelines Writing Committee (2024). 2024 ESC Guidelines for the management of chronic coronary syndromes. European Heart Journal.
Budoff, M. J., et al. (2007). Assessment of Coronary Artery Calcification by Computed Tomography: A Scientific Statement from the American Heart Association. Circulation
Narla, V., et al. (2020). High-Risk Plaque Features on Coronary CT Angiography. Current Cardiology Reports
American College of Radiology (ACR) / National Kidney Foundation (NKF) (2020). Guidelines for Intravenous Contrast Media Administration in Patients with Kidney Disease